Linus Pauling and others claimed that vitamin C is a highly effective cancer treatment when used correctly. They supported these claims with initial clinical trials that indicated an unprecedented increase in life expectancy. In addition, the initial results suggested a remedy far more potent than existing medicine could provide. Pauling was not the originator of these ideas but brought them to widespread attention. Here I will describe the high-dose vitamin C ideas as Pauling’s as it simplifies the explanation.
Linus Pauling, the Leading Chemist of the 20 Century
Pauling’s book about vitamin C and the common cold produced an unexpected backlash. Supposedly, Pauling, a scientific genius, had no right to present some minor ideas about vitamins and such a mild disease. He was vilified and accused of early senility. Corporate medicine argued that Pauling had no right to pontificate on areas outside his expertise. Their claims were bizarre as Pauling was one of the founders of molecular biology and the world’s most outstanding chemist. Pauling found their reaction informative. He realised this issue was vital and could stand modern medicine on its head.
Pauling based his claims for vitamin C and infections on huge intakes taken by mouth. But what about the major killers, such as cardiovascular disease and cancer? He went on to do preliminary clinical trials demonstrating outstanding cancer benefits. Since then, the National Institutes of Health (NIH) and others have confirmed the cytotoxicity of vitamin C. So the idea that vitamin C can be a potent cancer treatment is no longer controversial.
However, the NIH claimed that they had proven Pauling was wrong. They claim that only intravenously injected vitamin C can work. Purportedly, high-dose tablets are not absorbed. As Pauling realised, this is the core issue in human nutrition and has implications for the whole of medicine. Furthermore, it exposes a nonsensical medical pseudoscience at the heart of our society.
The mainstream attacked Pauling’s reputation just because he supported vitamin C. It was a warning. If they could publically denigrate one of the most outstanding scientists in history, lesser mortals had better watch out. Doctors and scientists quickly got the message. The suppression became so bad that nutrition “experts” and even major orthomolecular organisations now back the NIH low-dose claims and distance themselves from Linus Pauling. This endorsement is despite Pauling being the originator of orthomolecular medicine, which he described back in the 1960s. He used vitamin C to show the potential of his new ideas but presumably didn’t realise he was kicking a hornet’s nest.
Why did they attack Linus Pauling for suggesting vitamin C might help with the common cold?
Unfortunately for the NIH, studies on intravenous (IV) vitamin C and cancer have been underwhelming. They have not provided the same outstanding results as the early researchers who used mainly oral intakes. The cancer data suggest that supplements work and IVs don’t. Nevertheless, the focus shifted away from Pauling’s ideas, and the cancer industry remained exceptionally profitable. Look, a squirrel.
Following Pauling’s death, the NIH reported that oral vitamin C was not well absorbed. As a result, vitamin C could not have the properties Pauling said. Conveniently, Pauling was no longer able to defend his ideas. The US Institute Of Medicine also claimed that people only needed a small amount and based the recommended intake (RDA) on the NIH findings.

NIH Clinical Research Centre
We debunked the NIH work several years ago. Moreover, people widely acknowledged the errors. Indeed, the NIH work was considered a bad joke. The NIH should have withdrawn these papers or published a correction. But that would have been bad politics.
Since that time, the power and influence of the NIH have re-exerted themselves. The NIH is one of the largest sources of research funding. It does not pay to resist their influence. Do you want research funding? Then tow the NIH line and confirm only low doses of vitamin C supplements can be absorbed. Do you want your paper to get through peer review and past the editor? Then keep the faith. Professor Bruce Charlton’s book Not Even Trying: The Corruption Of Real Science describes the process well.
Promoting intravenous vitamin C and saying supplements can’t work serves several purposes. Primarily it removes a threat to big pharma as people don’t buy expensive drugs if they realise some cheap supplements are safer and more effective. Moreover, patients are in control of their own health with cheap oral vitamins. IV vitamin C is more profitable and returns the power to the clinic. It diverts people from looking at nutrition and other healthy alternatives to cytotoxic chemotherapy and radiation. Similarly, in an epidemic, people are directed away from prevention and home treatment to depend on doctors and patent medicines.
I will show in this series of posts that the official NIH recommendations are nonsense on stilts. Linus Pauling was correct. In my opinion, some leading “experts” are just scientifically incompetent. Either that or they want to play the official game to gain financial support and benefit their career.
That Awful Paper
The scientific corruption problem besets medicine in particular. Of course, intelligent readers will come to their conclusions, but I think the corruption will become obvious. On the other hand, if you are one of the “experts”, ask yourself if you really can risk continuing to support the NIH and their daft low-dose ideas as you read on. They are not only unscientific but dippy. When people find out, you will look stupid.
Doctors supporting the NIH claims for vitamin C can appear incompetent
Let’s start with the critical first NIH paper. Peer-reviewed papers about vitamin C are almost required to include a reference to this paper or state its findings. It is highly praised and was supposed to be uniquely rigorous. This praise is despite the public ridicule for its gross errors.
Here we go. The first figure in the paper includes this chart. It is blood levels of vitamin C measured after doses of oral vitamin C.
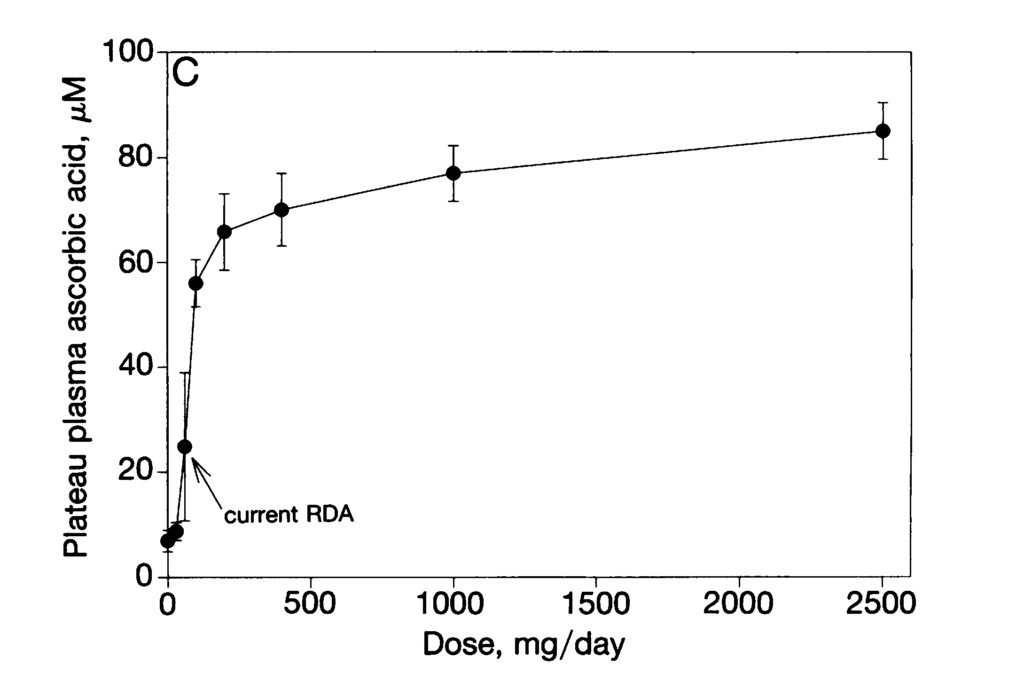
From Figure 1C in Levine et al
The idea was to find the smallest dose at which the blood plasma was at the maximum. Below this level, the body tries hard to hoard the vitamin. Remarkably, the NIH started with the right idea as if the body wastes vital energy to try to hold onto this level long term. We know you risk scurvy if you take very little, less than a few milligrams daily. However, we do not know if larger amounts prevent chronic disease.
So go ahead and find the data point (black disk) in their graph that gave the maximum blood plasma level.
Now we have a couple of school-level observations.
The maximum value was at the 2,500 mg dose, or two and a half grams in supplement speak. In other words, the NIH result entirely agrees with Linus Pauling. I have indicated the maximum by the big red arrow below to help the “experts”. This maximum is one that we might expect a schoolchild to find.
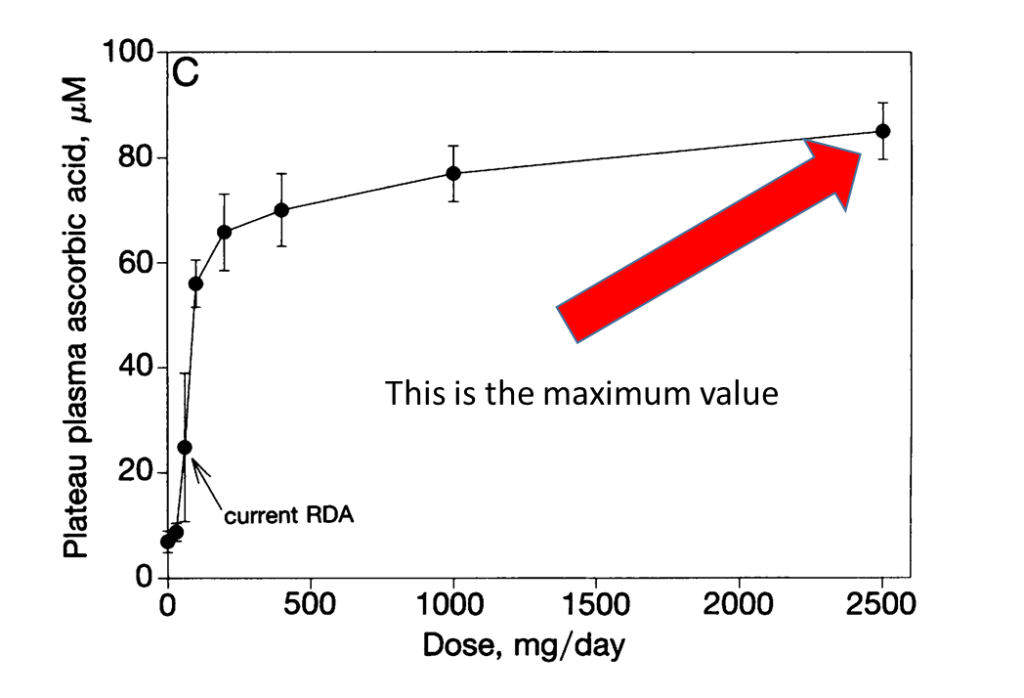
The largest measured value
However, look again. This measured maximum may indicate too low a value. The maximum blood level observed was at the highest dose given. Each larger dose produced a higher blood level. So it looks as if the real maximum is even higher. The trend suggests the blood level is still increasing at 2.5 grams. Judge for yourself.
The NIH data supports Linus Pauling
The increasing response may be why the NIH did not use higher doses. Extrapolating, it seems likely that the absolute maximum might occur somewhere between an intake of 3 and 5 grams. However, you can inspect the data and reach your own conclusions.
Telling A Story
People like stories. People trying to mislead often tell a story when they have an idea and the reality does not fit. They make up a good narrative and replace science with hype. It works. Stories are convincing for most people.
A good but irrational story can be convincing
So what’s the official story? Note the somewhat smaller red arrow in the chart below. Instead of selecting the maximum observed value, they chose one sufficiently close for the narrative. They selected a “near saturation” value as below. In other words, ignore the real maximum and choose a lower dose. A much lower dose. While the plasma level is still relatively high, the NIH “near saturation” selection drops the amount by about six times, from 2,500 to 400mg!
But notice they skipped a dose. The NIH needed to ignore another measurement because 1000mg still agreed with Linus Pauling’s gram levels. But now they focus on 400mg, which further helps their low dose argument. They could “sell” this as a good story and tell people Linus was wrong. But why stop there?
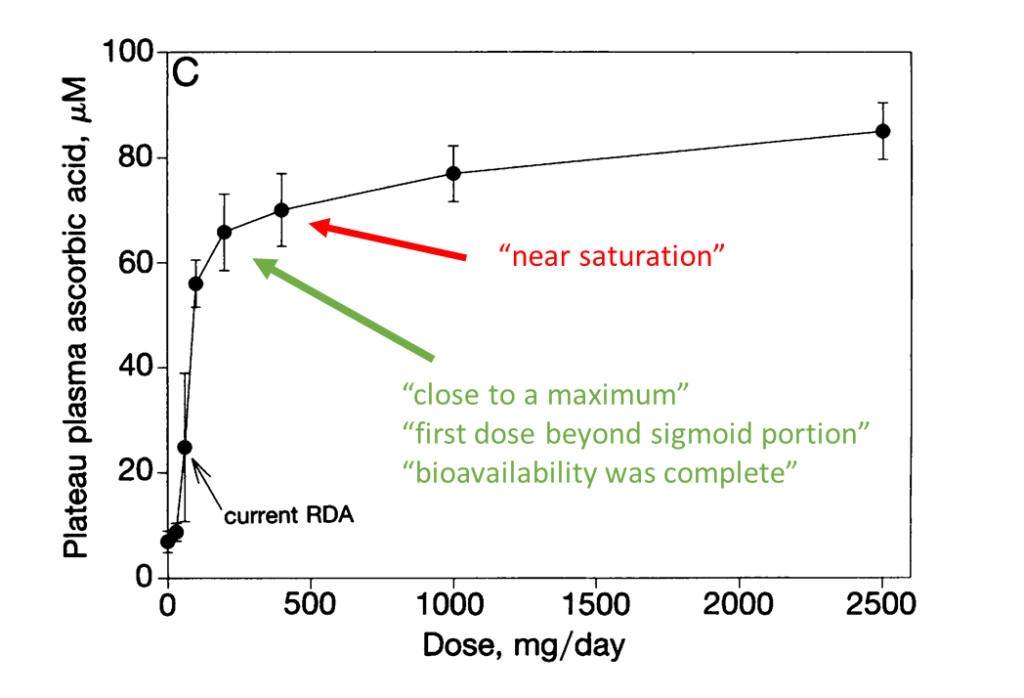
Going down to 200mg, they could say they had something “close to a maximum”. By sleight of hand, they now describe the 400mg “near saturation” point as some kind of maximum. Not THE maximum but A sort of maximum. The narrative has reduced the dose by more than 10x from 2,500 to 200mg! Now that’s a good story. But would anyone fall for it?
To support their case, they follow the lead of the extraordinary W.C. Fields who suggested the heuristic, “If you can’t dazzle them with brilliance baffle them with bullshit.” So the NIH invoked technobabble to support their case. They call the 200mg intake “first dose beyond the sigmoid portion”. The story is that many biological responses give an S-shaped curve, as here. In other words, after the initial fast start, 200mg is near where the S starts to lean over as the curve increases towards the top. Do you find this argument convincing? I thought we were trying to find the maximum blood level.
Continuing the technobabble in the narrative, we come to “bioavailability”. The NIH claims bioavailability is “complete” at 200mg. More weasel words? Bioavailability is what portion of a drug is absorbed. Complete bioavailability does not mean the maximum blood level or effectiveness. Lower doses absorb more easily than larger doses, as is generally the case with drugs. So the story becomes you get more bang for your buck with a dose of 200mg. Nonetheless, a 1mg dose absorbs better than a 50mg dose which absorbs better than a 100mg dose which absorbs better than a 1000mg dose. This idea is arbitrary. You could always choose a lower intake. In an extreme case, you could give so little and cause scurvy.
I could explain here that these data only apply to healthy young men. I was told they were volunteer medical students keen to work at the NIH. So the data does not apply to children, the elderly, the sick, or people who might have specific dietary requirements. Later I will describe how sick and stressed people absorb much more. Illness can turbocharge absorption. Doses of 100 grams a day can be absorbed by the sick. It will become apparent that the bioavailability and the intakes covered by the NIH have little relevance in such cases.
Here we have covered just one graph in the first figure of the silly NIH paper, which is a gold standard in the literature. However, I conclude that the NIH can’t even read a graph to the standard expected of a school science class. Medical science is in a parlous state if the errors in a so-called leading paper can be so dreadful and obvious, particularly if the mistakes have been highlighted for years.
But this is only part of Figure One. We will look at another detail of this figure in the next post. The errors just keep coming. Medicine’s acceptance of this nonsense is shocking.
Here is a short video to help the “experts” tell small from large when picking a maximum: