A sustained high blood level of vitamin C is a more effective anticancer agent than a short peak concentration. Most anticancer drugs are toxic, very toxic. They are slightly more poisonous to cancer than the host. The idea is to increase the dose to the maximum the patient can stand. The hope is damage to the tumour exceeds that to the patient.
Anticancer drugs with nasty side effects are not ideal as they initially grew out of chemical warfare agents. But back in the 1960s, it was realised that vitamin C could kill cancer cells, was safe, and essentially side effect free. The hope and expectations were that medicine would begin a new approach to treating cancer. However, cancer is highly profitable, with treatments costing thousands of dollars. So there was substantial resistance to the idea of an ideal anticancer agent that potentially cost mere pennies.
When Linus Pauling got involved, there was an opportunity for someone at the NIH to step in and sidetrack this potential cancer treatment. However, their experiments confirmed that vitamin C would kill cancer cells without harming the patient, which stymied a direct attack. This finding was terrible for marketing and not acceptable to the authorities. It would show that Linus Pauling and the others were right and modern medicine a sham. NIH politics needed a cover, so the NIH weaved a new storyline.
What if vitamin C needed to be at very high levels, only achievable by injection? Doctors could use this idea to take treatment out of the hands of patients, and inexpensive supplements would be no good. Corporate medicine might find this an acceptable result. Since it would show Pauling was wrong and agreed with the new low-dose RDA recommendations. They could incorporate it into chemotherapy showing how forward-thinking they were. Also, it would severely limit any benefit for the patient, as we shall see later.
The narrative that only IV vitamin C works was an easy sell. Doctors were in the mindset that the dose of anticancer drugs needed to be as high as possible. IV was a macho solution that appeared to be holistic and paid lip service to patients and doctors who believed in more natural therapies. Also, it fit the prevailing paradigm that vitamins were irrelevant and old news.
This interpretation is POSIWID: The Purpose Of a System Is What It Does. Don’t bother worrying about motivations, intent, or aims. Just ask what the system is doing. That is its purpose. In this case, the IV paradigm prevents a low-cost treatment where the patient is in control from interfering with the cancer business. Let’s get into the details.
Killing Cancer Cells
“The future of effective cancer chemotherapy will not rest on the use of host-toxic
compounds now so widely employed, but upon virtually host-non-toxic compounds, that
are lethal to cancer cells, of which ascorbate represents an excellent prototype.” Dean Burk 1969
We have known vitamin C is an effective anticancer agent for decades. For example, Dean Burk reported its properties in the 1960s. Its ability to kill cancer cells is not particularly controversial. Indeed, it has properties that put current cancer treatments to shame. It selectively kills cancer cells and is safe. In a sense, it has the characteristics of a magic bullet.
The establishment attacked Linus Pauling for merely suggesting vitamin C was of benefit in preventing the common cold. As you might expect, when Pauling and others researched the use of vitamin C in cancer, they were ignored or worse. However, the NIH work was lauded as a breakthrough when they did some me-too experiments and obtained similar results.
The NIH Misinterpret The Data – Again!
We can observe the utter gall of the NIH in the opening sentence “data indicate that i.v. ascorbic acid (ascorbate) in pharmacologic concentrations could have an unanticipated role in cancer treatment.” Unanticipated? Really? I was under the impression that many leading doctors and scientists had long since considered this an excellent hypothesis.

Ewan Cameron and Linus Pauling book published a decade before the NIH paper
Several doctors had published preliminary clinical studies showing that vitamin C helped cancer patients to survive longer. Many times longer than with current therapies. We will describe these reports later. But also notice that the NIH statement only refers to IV vitamin C. The NIH data didn’t study large oral intakes; they just excluded supplements by focussing on IVs. They claim that oral intakes cannot work, but their reasoning is spurious as we shall see. Oral intakes soak cancer for an indefinite time. So the effect of a short exposure would not reflect the potential of supplements.
We will once again use the NIHs own data to show their errors. Here is a chart from the influential NIH paper.
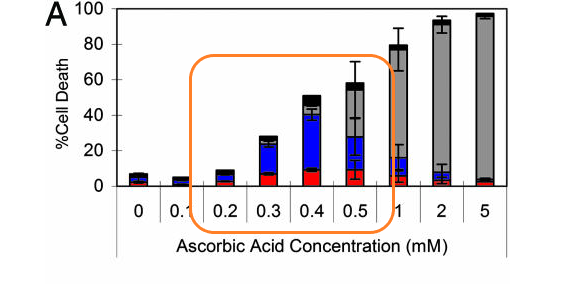
The chart shows cancer (Burkitt’s lymphoma) cell death compared with the concentration of vitamin C (ascorbic acid). The different colours roughly indicate the way the cells died. Blue and red indicate controlled cell death (apoptosis) which is ideal. Black (necrosis) and grey (pyknosis/necrosis) are uncontrolled and should be avoided where possible. Thus, the colour coding indicates that the ideal vitamin C level would be around 400 microM (0.4 mM). Higher levels kill more cells but in a less desirable way.
Oddly, the NIH seemed most interested in cell death approaching 100%, which required 2,000 microM (2mM in the chart). This restriction seems reasonable at face value until you realise that the NIH treated the cells with vitamin C for only one hour. Why for such a short time? Because an IV will only last a few hours. The NIH had prejudged the results.
Linus Pauling and others were not interested in killing cancer in an hour or two of treatment. Kill cancer too quickly, and you stress the body. The tumour might bleed. Moreover, the body needs to clean up all those dead cells, biological sludge, and other crud. Otherwise, you have a major toxic shock. More practically, a process that kills a few per cent of the cells daily is preferred. The body can then eliminate the trash without toxicity.
I have indicated the blood levels people can obtain with supplements with the orange window in the chart. Notice this single hour of treatment generates about 10% cell death at 200 microM (0.2mM), 30% cell death at 300 microM (0.3mM), 50% cell death at 400 microM (0.4mM), and 60% cell death at 500 microM (0.5mM). This blog series shows that these levels are sustainable using oral liposomal supplements.
Selective Killing of Cancer
Here is another representation of the NIH data. The upper curve shows the percentage of cancer cells killed. The two lower curves show the minimal, if any, effect on normal white blood cells. The NIH used this data to confirm the selective cancer-destroying properties of vitamin C. Remember, this work was just more me-too replication. But a reader of the paper might not realise this as Dean Burk’s and other relevant articles were not referenced.

The NIH aimed to find out if “pharmacologic concentrations kill cancer cells, but not normal cells, using conditions that mimic i.v. use and a clinically relevant time course?” So let’s unpack the statement. Firstly, we already knew high levels of vitamin C kill cancer cells but not normal cells. So they should also have known this fact, but there was no harm in replicating the earlier work. It is, however, usual to put your work in context by referencing earlier scientists.
Then the NIH was interested only in IV treatment. They would ignore oral doses or claim that they would not work. They present no data to show that this is true. Indeed, their data indicates the opposite. They provide a rising curve with 0.5 mM (500 microM), which causes 60% cell death after one hour of treatment. Also, we have covered how it is possible to sustain levels at or above 500 microM (0.5mM) using oral intakes.
Indeed, we have seen data suggesting a single gram of well-formulated liposomes can generate almost 300 microM/L. This concentration corresponds to 30% cell death in the NIH study. From the data people have provided to me, liposomes combined with standard supplements can produce blood levels of around 700microM or more. We can appreciate this immediately, as liposomes and ascorbic acid absorb by different mechanisms.
Then the NIH have another restriction. They are only interested in what they describe as a clinically relevant time course. That is how well vitamin C can kill cancer cells in a short IV treatment. In this case, over a single hour. IV treatment usually occurs in a short interval measured in hours. Do I need to explain that treatment might kill more cancer cells if extended to two hours, two days, two weeks, or two years? The dead cells could not be fewer because they could not come back to life!
One Way It Works
It had been known for years that vitamin C could generate hydrogen peroxide (H2O2). This exciting finding is because the vitamin usually acts as an antioxidant but as an oxidant in tumours. We will come back to this process later.
Notably, we have known that hydrogen peroxide could kill cancer cells for years. In 1957, a friend of mine, Dr Reg Holman, published a report on this in Nature. Reg reported cancerous rats surviving. His preliminary results suggested that “the rate of cure is on the average 50-60 per cent.” As you might expect by now, the NIH did not reference earlier work on peroxide and cancer by Holman and others.
Grace Jeffree partly replicated Reg’s observations. “Drinking hydrogen peroxide thus appears to have two effects on the tumour-bearing rat. It slows down [tumour] growth by reducing food and liquid intake, and it tends to raise the catalase/haemoglobin ratio in the blood. No effect on survival was found in this experiment.” These are also fascinating and unexpected results as the enzyme catalase should prevent peroxide from reaching the tumour. However, if you can get the peroxide to the tumour, it is an effective anticancer agent with little toxicity to the host. Vitamin C has these local properties.
Unfortunately, a research group from Sheffield claimed to know better and responded with a sarcastic letter to Nature. They also tried to replicate Reg Holman’s experiment – poorly. For example, they used a different type of tumour but claimed it was “in an exactly similar experiment”. This response and Holman’s challenge to the status quo led to the repression of his work.
For interest, I can access Reg Holman’s laboratory notes and results. His results might have been a statistical fluke. However, there is a potential explanation for Holman’s positive findings. There are some direct hints he communicated to me, backed up by his lab notes. It seems he could have used a catalase inhibitor. Catalase is an enzyme that breaks down H2O2. However, Reg could be difficult and would have been unlikely to help those he perceived as antagonistic by giving away his secrets.
Once again, doctors don’t attack the NIH. So let’s not be too gullible. When the NIH says peroxide kills cancer, their funded researchers and the medical journals fall into line.

These two graphs show the NIH data on the effect of hydrogen peroxide on cancer cell survival. Vitamin C may work in part by generating peroxide. However, remember the process is selective, and the peroxide is generated locally by vitamin C acting as an oxidant. In most healthy tissues, it acts as an antioxidant.
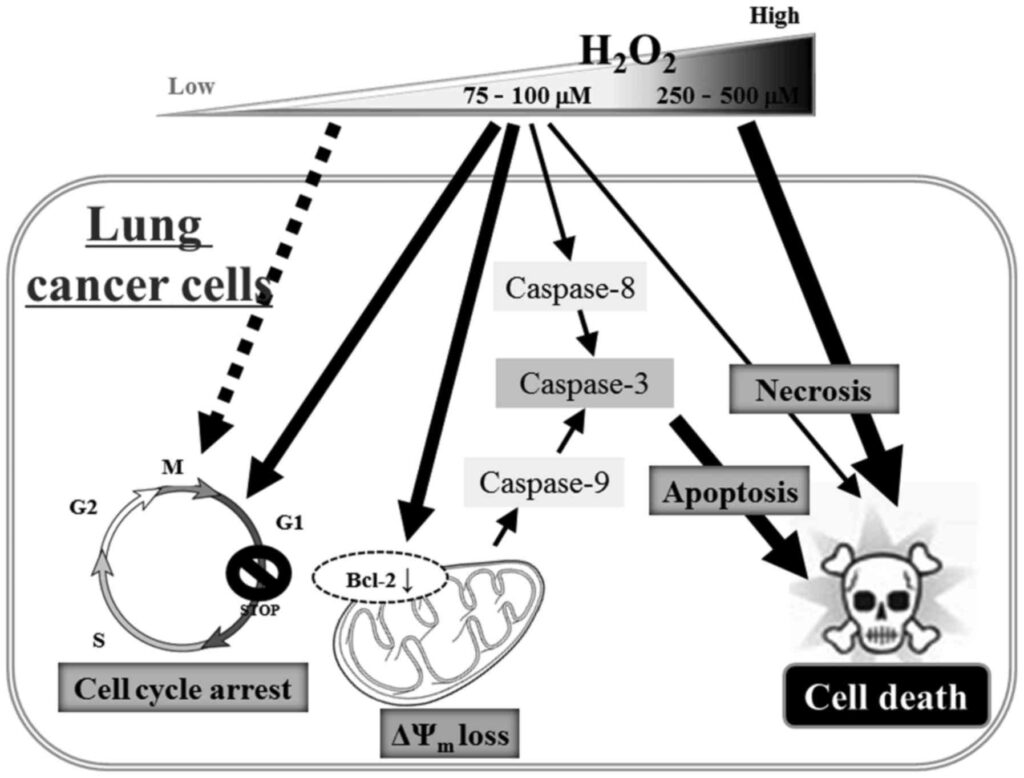
A diagram of some of the mechanisms for hydrogen peroxide in cancer from more recent research is shown below. Taking hydrogen peroxide is not advisable because “it is a deadly poison”, as Holman stated. However, vitamin C supplements used intelligently target tumours with peroxide while sparing healthy tissues.
Medicine lost decades by ignoring Reg Holman and the vitamin C crowd.