Vitamin C can enable cancer patients to live longer. At least, that’s what the data from the initial clinical trials demonstrate.
To gain context, we will consider the big cancer killers, solid tumours in major organs. Lung, breast, colon, rectal, stomach, kidney, ovary, and bladder cancers are well-known examples. Doctors consider most conventional cancer chemotherapy successful if it helps a small percentage of these patients. However, patients gain minor benefits at the cost of severe side effects and loss of wellness.
Cameron and Pauling
We will begin with Ewan Cameron, a Scottish surgeon and Linus Pauling. Their results were outstanding. They noted that cancer patients were short of vitamin C and might need an increased intake to fight the illness.
The first thing to note is the 1974 paper by Cameron and Campbell, “The orthomolecular treatment of cancer. II. Clinical trial of high-dose ascorbic acid supplements in advanced human cancer”. I have highlighted the word “supplements” in the title. The wording will be important when considering the NIH claims for IV.
In 1974, Cameron and Campbell reported the response of 50 consecutive cancer patients to high-dose vitamin C supplements. They said supplementation was safe and of definite value in terminal cancer. Furthermore, they suggested that it might support earlier, more favourable cases. These are hardly earth-shattering conclusions and should not have been controversial.
Cameron and Pauling continued the reports and, in 1976, described 100 patients given 10g of vitamin C supplements as part of their routine therapy. They compared them to 1,000 matched control patients who they gave no vitamin C. The controls lived an average of 50-days. Those taking vitamin C lived over four times as long (210 days). For nine patients out of 10, the vitamin C slowed the death rate to a third. The remaining 10% of patients lived more than 20 times longer than the controls. Rather modestly, they suggested that “the results clearly indicate that this simple and safe form of medication is of definite value in the treatment of patients with advanced cancer.”
Here is their graphical summary of data for four primary cancers:
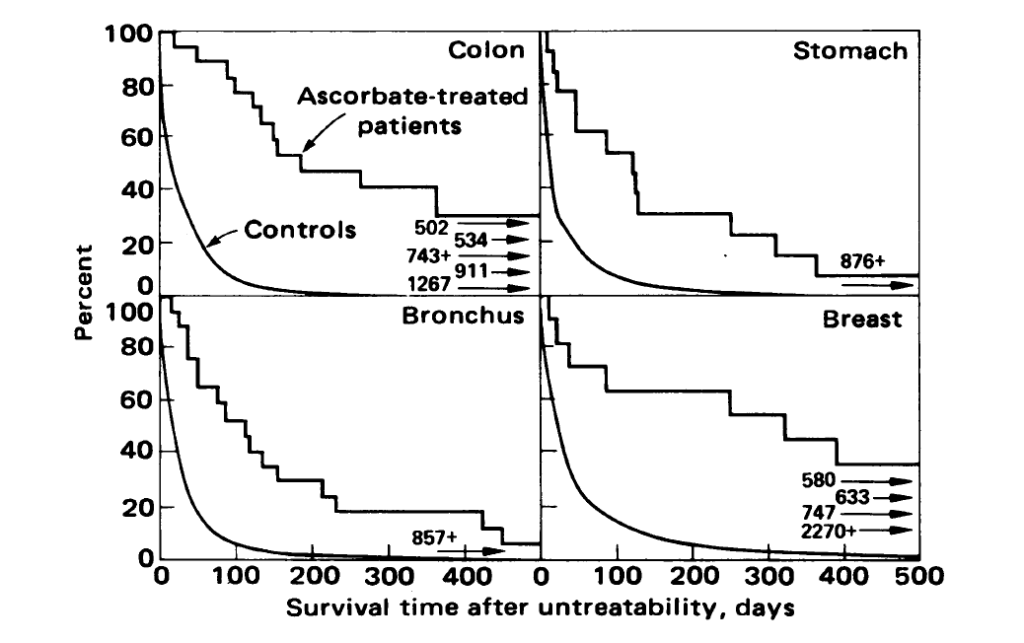
It should be immediate that the vitamin C (ascorbate) treated patients lived far longer than the controls. The numbers and arrows give results for subjects who lived too long to fit on the chart. These values are for vitamin C treated patients. The increased survival occurs in colon, stomach, bronchus, and breast cancers. What is not apparent from the data is that these results were outstanding. The patients were terminal, and there was no other treatment available. Despite this, vitamin C extended their lives far more than conventional treatments.
Not Poor Experimental Design
Of course, the immediate claim was that this was not a good experiment, as it didn’t randomise the patients. Nevertheless, it was supposed to be an initial test of the hypothesis, which required sensible replication by others. We will later see that conventional medicine could not repeat the trial because of its bias and a fundamental lack of competence.
It is interesting to note something technical at this point. Consider the first graph for colon cancer. The treated patients have died by about 300 days. The paper’s raw data showed that the longest-living colon control patient lived 224 days. At this time, about 40% of the treated group is remaining. After 500 days, there are about 25% remaining, and several lived far longer. So how could you select the longest-lived treated subjects from the control group?
This limited potential for selection is vital, as one of the later criticisms was that Cameron-Pauling could have somehow chosen long-lived patients to receive vitamin C. However, selection is an impractical explanation for the results. For a start, it appears that the first 50 treated patients were consecutive. Look at the graph. After 224 days, there are no colon control patients left alive. Selecting people living 502, 743, or 1,267 days from the controls would not be possible. How could you pick a person who lives 1,267 days (3.5 years) from a group who are all dead after 224 days (7-8 months)? This difficulty should be evident from just looking at the chart.
Look at all four graphs. Do you think that you could select the long-lived treated from the short-lived controls? I think not. However, I have done some back-of-the-envelope statistical calculations and selecting long-living patients for treatment is impractical. The readers of a mathematical bent can confirm this themselves.
If we play the selection game, we need to know which terminal patients to select for treatment in advance. Unfortunately, doctors are not able to predict cancer longevity accurately. In this case, the doctor would need to have near-perfect judgement and select a group of at least 50 consecutive patients who would live longer at the start of the experiment. The results are so disparate that we can rule out selection errors.
Further Results
Cameron and Pauling reported a further four groups of tumours with similar results.

Once again, the results were astounding. We can see visually that ovarian cancers were less responsive. Indeed, we could probably manage to select the most long-lived ovarian patients from a large group of controls. However, results from these four cancers are similar to those from the earlier graphs.
Critics
Cameron and Pauling responded to criticisms of their work in 1978. They used an updated set of controls and addressed some technical objections. The results were similar. They were trying hard with the resources available to have doctors do clinical trials. Despite their standing, the importance of the work, and popular support, they could not perform a full-scale randomised clinical trial of the form required by their critics. Note the title of this later paper is “Supplemental ascorbate in the supportive treatment of cancer.” You will note I have once again highlighted the word “supplemental”. Now, what does this word suggest to you?
For fun, I did an online image search on “supplemental vitamin C” and obtained page after page of pictures of tablets and other oral forms like this:

Supplemental vitamin C
Cameron and Pauling would have specified IV if they were not discussing supplements. In Ewan Cameron’s own words
“The intravenous regime is probably unnecessary as a routine measure, and need only be employed in clinical situations, where vomiting, anorexia, or other complications of malignancy preclude oral administration.”
The NIH would later claim that Cameron and Pauling obtained such great results because they used IV vitamin C! They cherry-picked data from the few examples of IV described by Cameron. This claim was an attempt to support the mainstream and promote their misunderstanding of vitamin C pharmacokinetics.
Cameron had tried IV vitamin C in some patients but found it unnecessary. We will see later how others obtained exceptional results with oral but not IV vitamin C. Unfortunately, to my knowledge, IV vitamin C studies have not provided similar benefits to Cameron-Pauling in cancer. This failure is expected from pharmacokinetics, mainly how oral doses are absorbed and sustained in the body.
Corporate medicine treats vitamin C as a threat. But Cameron and Pauling were not promoting a cure for cancer, just a better treatment. One that kept patients alive for longer and helped them feel better. I will show later how vitamin C’s anticancer action can be supercharged with symbiotic supplements.
Interested readers can find more details of Cameron and Pauling’s work in their book:
